184. Save Your Kidneys
Vesicoureteral Reflux (VUR)
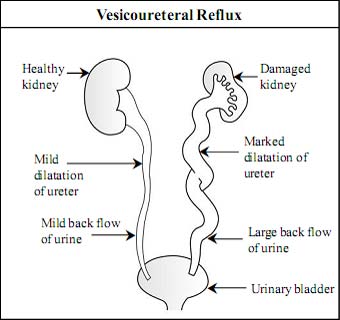
Vesicoureteral reflux (VUR) is “backward flow of urine from bladder into ureter”.
Why is it important to know about vesicoureteral reflux?
VUR is present in about 30 to 40 % of children with UTI associated with fever. In many children VUR may cause scarring and damage to the kidneys. Kidney scarring for a long period may cause high blood pressure, toxemia of pregnancy in young females, chronic kidney disease and, in a few patients, end stage kidney disease. VUR is more common in family members of a person with VUR and affects girls more frequently.
What is vesicoureteral reflux and why does it occur?
VUR is a condition with an abnormal backward flow (reflux) of urine from the bladder toward the ureters and possibly up to the kidneys. This can happen on either one or both sides.
Urine formed in kidneys flows down to the urinary bladder through the ureters. Urine normally flows in one direction, down the ureters and into the urinary bladder.
During urination and when the urinary bladder is filled with urine, a valve between the bladder and ureter is responsible for the prevention of back flow of urine into the ureters. VUR is caused by a defect in the mechanism of this valve.
VUR can be graded from mild to severe (Grade I to V) based on the severity of back flow of urine from the urinary bladder to the ureters and kidneys.
VUR is very common in children with UTI and carries the risk of hypertension and CKD.
CHP. 23. Urinary Tract Infection in Children 185.
 What causes vesicoureteral reflux?
What causes vesicoureteral reflux?
There are two types of VUR: primary VUR and secondary VUR. Primary VUR is the most common type of VUR and is present at birth. Secondary VUR can occur at any age. It commonly occurs due to obstruction or malfunction in the bladder or urethra with bladder infection.
What are the symptoms of vesicoureteral reflux?
There are no specific signs and symptoms of VUR. But frequent and recurrent urinary tract infection (UTI) is the most common presentation of VUR. In older children with untreated severe vesicoureteral reflux, signs and symptoms are apparent because of complications such as high blood pressure, protein in urine or kidney failure.
How is vesicoureteral reflux (VUR) diagnosed?
Investigations performed in children with suspected VUR are:
1. Basic diagnostic test for VUR
Voiding cystourethrogram
- VCUG is the gold standard for the diagnosis of vesicoureteral reflux and its severity (grading).
- Vesicoureteral reflux is graded according to the degree of reflux. The grade of VUR indicates how much urine is flowing backward into the ureters and kidneys. Grading is important in determining prognosis and most appropriate therapy for a given patient.
- In the mild form of VUR, urine refluxes only to the ureter (Grade I and II). In the most severe form of VUR there is massive reflux of urine, with marked tortuosity and dilatation of the ureter and severe kidney swelling (Grade V).
2. Additional investigations in VUR
- Urine test and urine culture: used to detect a urinary tract infection.
- Blood tests: basic tests usually performed are hemoglobin, white blood cells and serum creatinine. Serum creatinine can be used as a measure of kidney function.
- Kidney and bladder ultrasound: to find out the size and shape of the kidneys and to detect scars, kidney stones, obstruction or other abnormalities. It cannot detect reflux.
- DMSA kidney scan: this is the best method for detecting kidney scarring.
How is vesicoureteral reflux treated?
It is important to treat VUR to prevent possible infections and kidney damage. The management of vesicoureteral reflux depends on the grade of reflux, age of children and symptoms. There are three treatment options for VUR, : antibiotics, surgery and endoscopic treatment. The most common first-line treatment of VUR is the use of antibiotics to prevent UTI. Surgery and endoscopic treatment is reserved for severe VUR or in those cases where antibiotics have not been effective.
With regular antibiotics for a long term (years), low-grade reflux resolves without surgery.
CHP. 23. Urinary Tract Infection in Children 187.
Mild VUR: Mild VUR will resolve completely on its own by thetime a child is 5 to 6 years old. Children with mild VUR are less likely to need surgery. In such patients, a low dosage of antibiotics is given once or twice a day for a prolonged period of time to prevent UTI. This is called antibiotic prophylaxis. Antibiotic prophylaxis is usually given until the patient is 5 years of age. Remember that antibiotics per se do not correct VUR. Nitrofurantoin and cotrimoxazole are preferred drugs for antibiotic prophylaxis.
All children with VUR should follow general preventive measures for UTI (discussed above) and regular frequent and double voiding. Periodic urine tests are needed to detect UTI. VCUG and ultrasound are repeated yearly to determine if reflux has subsided.
Severe VUR: The severe form of VUR is less likely to resolve on its own. Children with the severe form of VUR require surgery or endoscopic treatment. Correction of reflux by open surgery (ureteral reimplantation or ureteroneocystostorny) prevents the backflow of urine. The main advantage of surgery is its high success rate (88-99%). Endoscopic treatment is a second effective treatment modality for the severe form of VUR. The benefits of endoscopic technique are that it can be performed in an outpatient setting, takes just 15 minutes, has fewer risks and does not require any incision. Endoscopic treatment is done under general anesthesia. In this method with the help of an endoscope (lighted tube) a special bulking material (e.g. Dextranomer/ hyaluronic acid copolymer - Deflux) is injected into the area where the ureter enters the urinary bladder. Injection of the bulking material increases the resistance at the entry of the ureter and prevents urine from flowing back into the ureter. The success rate for resolution of reflux with this method is about 85 to 90%. Endoscopic treatment is a convenient treatment option in the earlier stage of VUR as it avoids long term use of antibiotics and the stress of living with VUR for years. Follow-up:All children with VUR should be regularly monitored with measurement of height, weight, blood pressure, urine analysis and other tests as recommended by his/her doctor.
Surgery and endoscopic treatment are indicated in severe VUR or when antibiotics are not successful.
188. Save Your Kidneys
When should a patient with UTI consult a doctor?
For children with urinary tract infection the doctor should immediately be consulted in case of:
- Persistent fever, chills, pain or burning during urination, foul-smelling urine or blood in the urine.
- Nausea or vomiting which prevents intake of fluid and medication.
- Dehydration due to poor fluid intake or vomiting.
- Pain in the lower back or abdomen.
- Irritability, poor appetite, failure to thrive or child is unwell.
Regular follow up is advised in VUR to assess blood pressure, growth, recurrence of UTI and damage to the kidneys.